22 Feb 2016
Dental imaging in horses: part 2 – advanced and oral techniques
Tim Barnett
Job Title
Figure 1. An oral endoscopic view of the occlusal surface of a mandibular cheek tooth with loss of secondary dentine and exposure of the pulps.
As discussed in part one of this article (VT46.04), thorough oral examination with an illuminated mirror and radiography are the mainstays of investigating suspected equine dental disease.
However, as in many other body systems, the findings of such examinations are often equivocal, so further diagnostic techniques and imaging modalities are often indicated.
Oral endoscopy


Most pieces of equipment allow magnification of the images, which is particularly useful when looking for subtle changes, such as pulp exposure (Figure 1) or fissure fractures (Figure 2). Additionally, most modern oral endoscopes are attached to photographic or video recording devices that allow the clinician to create records of the clinical findings.
In addition to being an essential diagnostic tool, oral endoscopy has become invaluable as a means of observing and guiding surgical procedures in the mouth.
Oral endoscopy is most conveniently performed in the sedated patient, both for ease of use and safety of the patient and equipment, following the placement of a routine oral speculum. A tongue retainer (Figure 3) is often useful to allow unimpeded placement of the endoscope and prevent it being moved by the tongue and the cheeks during examination.
A systematic approach ensuring complete examination of the mouth should be developed, ensuring the occlusal, buccal and lingual/palatal aspect of all four cheek tooth arcades are included. The periodontal tissues should be inspected, as well as the teeth. Other oral soft tissues can also be inspected, and recording of images of buccal ulceration (Figure 4) and tongue trauma provide useful means of client education.
Scintigraphy
Nuclear scintigraphy involves intravenous injection of a radiopharmaceutical (“radiolabelled agent”), and the standard agent used for bone phase imaging in horses is technetium-99m (99mTc). In equine dental imaging, it is usually changes in the bone surrounding the teeth that are investigated and, for that reason, it is most readily bound to methylene diphosphonate or hydroxymethylene diphosphonate. Both these substances then bind to hydroxyapatite in bone and are concentrated in regions of elevated osteoblastic activity.
The concentrated 99mTc emits gamma radiation, which is detected by a gamma camera. A computer converts this into the diagnostic image. Lateral and dorsal views are usually obtained from the standing sedated patient, but, in some cases, oblique views and more specific focal views may be necessary.

Scintigraphy is unique among the more commonly used imaging modalities because the images represent active physiological processes rather than the structural features shown by other forms of imaging. MRI also has this advantage, but is used infrequently in equine dental examinations.
Scintigraphy can, therefore, detect changes in bone that precede radiographic changes, which makes it useful in the diagnosis of early apical infection. It is also particularly useful in cases of suspected infections of supernumerary or dysplastic teeth, where the results of radiography, or even CT, may be unclear.
Apical infections of the cheek teeth typically result in focal and intense increased radionuclide uptake (IRU) located in the periapical region of the affected tooth. When partnered with radiography, a high sensitivity and specificity for detection of periapical infections is achievable (Figure 5; Weller et al, 2001).
Scintigraphy is also useful for differentiating primary and secondary sinusitis cases, with the IRU more diffusely distributed throughout the sinuses in cases of primary sinusitis. However, some cases of primary sinusitis have been reported that are characterised by a focal area of IRU that could easily be mistaken for periapical disease (Barakzai et al, 2006). Careful use of a number of views may help to differentiate such findings.

Similarly, fractures of the skull may cause intense regions of IRU (Barakzai and Barnett, 2015) that may overlay tooth apices, leading to confusion. Use of scintigraphy in imaging postextraction complications is limited, as the alveolus can have IRU for up to 24 months following tooth removal (Barakzai and Barnett, 2015).
Despite these benefits, scintigraphy does not allow direct visualisation of anatomy and the images produced are inherently low resolution. In addition, scintigraphy has relatively expensive initial setup costs and the daily running is labour-intensive. Scintigraphy also necessitates the use and storage of unsealed radioactive materials and waste, which is governed by complex legislation. Despite this, and due to its invaluable use in upper limb and spinal orthopaedic diagnostics, it is a more widely available than other advanced techniques, such as CT.
CT
CT uses multiple differential x-ray beams, which are collected by a tube detector that rotates around the long axis of the horse’s head. The data is collected and greyscale values assigned based on the attenuation by the tissues examined. Using computer software, tomographic slices of the area imaged are created and displayed on a monitor.
Subsequently, multiplanar reformatting and three-dimensional reconstructions of the original data set can be performed to assist image interpretation.

CT has an inherently higher contrast resolution when compared to conventional radiography and scintigraphy, allowing a more accurate differentiation between tissue types, such as soft tissue and fluid. CT is a “cross-sectional” technique, negating problems caused by superimposition, which are ubiquitous to head and oral cavity radiographs. The images can also be optimised for evaluation of the different tissue types – bone, dental tissues and soft tissues.
Units of measurement (Hounsfield units; HU), based on the linear attenuation coefficient of the tissues in each voxel relative to the attenuation value of water, have been assigned to most tissues. Determination of certain tissue types can be made using the HU values obtained in clinical cases.
Fluids can often be distinguished from soft tissues due to the high contrast resolution and, in some cases, the differing HU can differentiate between fluid types.
Most CT units in use for equine work are adapted from human systems, with the table being modified to allow the horse’s head to pass through the gantry as the table moves or, in some cases, as the gantry moves over the table. Prior to the pioneering skills of the late Alastair Nelson MRCVS, most CT examinations of the head necessitated general anaesthesia.
Mr Nelson designed and developed a custom-made platform system specifically for imaging horses under standing sedation that can be attached to the conventional (human) patient bed. These systems have been developed further, but most still use the original air skate design, allowing frictionless, zero inertia movement of the patient through the gantry.
Preparing and positioning the horse takes time and patience, but the scan time is extremely fast – about 30 seconds to image the whole head. The standing procedure is occasionally not possible in nervous or head shy horses, and size limitations exist (very large or very small horses may be difficult to position within the gantry).
However, there remains the option to perform the scan under general anaesthesia in dorsal recumbency using a similarly modified anaesthesia table.
The anatomy of the equine cheek tooth is complex, with different tissues having varying attenuations, thus allowing the detailed anatomy to be appreciated using CT. The infundibulae of the maxillary cheek teeth is one area that comes under much scrutiny by some clinicians, as infundibular hypoplasia and caries formation can be implicated in secondary dental disease, such as fractures or periapical infection.
Infundibular cemental hypoplasia and caries are very common (65 per cent; Windley et al, 2009) in the horse and, unless particularly severe and breaching the infundibular enamel, they are often considered as normal variations (Veraa et al, 2009; Windley et al, 2009). CT examination has proved to be more sensitive in the determination of the severity of infundibular caries in comparison to oral examination (Veraa et al, 2009), as it allows visualisation of the subocclusal cemental defects in addition to the infundibular enamel.

In those cases necessitating restoration, CT provides the surgeon with some guidance of the depth and shape of the defect. Pulp horns are evident on CT image as distinct hypoattenuated structures within the teeth, which decrease in diameter with advancing age as more secondary dentine is deposited in the horns. Apical foramina can also be observed on CT, which also reduce in diameter with age. As with radiography, the indistinct root formation in the juvenile tooth can be appreciated on CT examination.
Determining periapical infections is the most common reason for CT examination of the equine oral cavity. CT has proven to be more sensitive than radiography – not just by eliminating superimposition of overlying structures, but also by allowing the recognition of subtle and earlier changes. Expansion and disruption of the alveolar bone can be identified, along with loss of the lamina dura and widening of the periodontal space in cases of periapical infection (Figure 6).
Pulp stones and gas can be identified in the pulp horns, along with increased diameter and irregular margination of the pulp horns (Buhler et al, 2014). In more chronic cases, destruction of the apices and cemental proliferation can also be identified on CT – seen as clubbing and fragmentation of the roots.
Success of potential endodontic treatment is likely dependent on the pulp morphology and health; thus, thorough CT examination of the teeth is advisable in these cases.
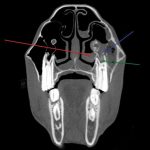
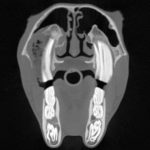
CT is particularly useful in differentiating cases of dental sinusitis, with the CT findings of a periapical infection being present along with the signs of sinusitis (Figure 7). These include a thickened sinus mucosa, fluid with the sinus lumen, inflammation and thickening of adjacent bones, subcutaneous soft tissue swelling, and remodelling of the nasal conchae (Henninger et al, 2003; Barakzai, 2012). Purulent and food material can also be identified, which gives a characteristic heterogenous attenuation in the lumen of the sinus (Figure 8; Barakzai and Barnett, 2015).
CT is useful in determining the anatomy of misaligned, dysplastic and supernumerary teeth (Figure 9), as well as dental and dental-related tumours. CT is especially useful in the investigation of postextraction complications, with accurate determination of dental remnants, sequestrae and orosinus fistulae.

MRI
Similar to CT, MRI allows the generation of cross-sectional images of the equine head and dentition. MRI has the unique feature of all the techniques available for imaging horses of representing both the physiologic and anatomic nature of tissues. The images are generated from the varying signal intensities emitted from the hydrogen nuclei in the tissues of the head and does not use ionising radiation. No systems are capable of imaging the equine head without the need for general anaesthesia, and anaesthesia times are prolonged (one to two hours) compared to CT (15 minutes).
MRI is particularly useful for imaging periodontal soft tissues, with much greater contrast resolution and sensitivity than other modalities such as CT. Sequences have been developed allowing accurate diagnosis of endodontic disease – in some cases necessitating the use of contrast.
Due to the necessity for general anaesthesia and the limited availability of MRI scanners that can accommodate the equine head, its use is, at present, limited in equine dentistry.
Acknowledgments
The author would like to acknowledge Safia Barakzai, Marcus Head, Sarah Powell and Pete Ramzan.
Latest news
