10 Jan 2023
Challenges in eyelid surgery
Ron Ofri PhD, DECVO, DVM outlines how various conditions – including entropion, ectropion and tumours – can be treated surgically.
Ron Ofri
Job Title
Figure 1. Normal anatomy of the eyelid in a dog. Note that you can see the entire length of the lower eyelid margin in firm contact with the globe, implying that no entropion or ectropion is present. The tear film meniscus can also be seen between the lower eyelid and globe, another sign of proper lid anatomy and function.
Eyelids may be affected by many skin diseases and patients may present with common dermatological signs, such as alopecia, erosions and ulceration, crusting, pruritus and so forth. These are usually treated medically, following work-up according to dermatological guidelines.
But other eyelid diseases – including traumas, such as eyelid laceration, tumours, and most commonly inherited eyelid abnormalities that affect normal eyelid anatomy and function in many dog breeds – can only be treated surgically.
However, the eyelids are a delicate piece of skin and the surgeon must restore proper eyelid anatomy, which is essential for protection of the globe, as well as for distributing the tear film on the ocular surface (Figure 1). This article reviews surgical correction of several common disorders of this important organ.
Entropion

Entropion, or inward rolling of the eyelid margin, causes eyelashes and facial hair to contact the conjunctiva and cornea (Figure 2), leading to excessive tearing, pain, conjunctival hyperaemia, keratitis and possible ulceration.
Entropion may be cicatricial (due to scarring from an injury or previous surgery) or spastic (due to contraction of the orbicularis oculi muscle). However, in dogs it is most often conformational and/or inherited, with scores of predisposed breeds, including many brachycephalic and retriever breeds, as well as the chow chow, English bulldog, Irish setter, St Bernard, Shar Pei, Rottweiler and great Dane. Many patients will present with bilateral entropion, most commonly of the lower eyelids, although the length of affected eyelid may vary. For example, in large, broad-skulled breeds, entropion often affects the lateral canthus and lateral part of the lower eyelid, while in brachycephalic breeds, the medial lower eyelid is commonly inverted.
In breeds with heavy facial folds, such as the bloodhound, Shar Pei and chow chow, the upper lids are often affected.
In some cases, patients may present with entropion at a very young age. You may wish to delay the surgery due to anaesthetic risks in puppies, and also because the entropion may diminish or even resolve as the animal matures.
In such cases, you could alleviate the pain and prevent corneal irritation with temporary tacking. Tacking can also be used in cases of temporary entropion due to transient enophthalmos caused by dehydration or lack of orbital fat, or when a primary, treatable cause for spastic entropion is present (such as a corneal ulcer). Staples are preferred to skin sutures, as they are less traumatic and can be quickly placed in an alert or sedated patient, without general anaesthesia (Figures 3a and 3b). They may be applied several times as the puppy grows and until it reaches maturity.
In recent years, subdermal injections of hyaluronic acid filler have also been advocated as treatment for entropion. These injections are also performed without anaesthesia and, therefore, are suitable for patients who are anaesthetic risks. They are longer lasting than staples, as a mean follow-up time of 194 days has been reported, but, unlike staples, the injection may be irreversible.
Surgical correction
Make sure that underlying causes, such as corneal ulcers or dehydration, as well as any blepharitis have been treated prior to surgery.
Next, in the awake dog, estimate the amount of skin that needs to be removed.
Apply topical anaesthetic, and use your fingers to roll out the eyelid until its margin (meibomian gland orifices) can be seen along the whole lid length; this will assist in outlining the full lateral and medial extent of the entropion.
Most cases of simple entropion are treated using the modified Hotz-Celsus procedure. Make your first incision parallel to the eyelid margin about 2.5mm from the margin, while protecting the ocular surface with a lid plate. If your incision is too close to the margin, you will not have enough skin through which to pass your sutures; if too far, you will achieve less eversion when suturing.
The incision should extend 1mm laterally and medially beyond the extent of the inverted eyelid. Continue the incision by making a curvilinear cut joining the two ends of this first incision, so you end up removing a crescent-shaped piece of skin. The thickness of the crescent (that is, the vertical distance between the two incisions) should have been predetermined during the examination of the awake patient and confirmed during surgery with your digital eversion.
In chronic cases, lid alopecia and discolouration will also indicate the amount of skin that needs to be removed. Use scissors to dissect the skin from the underlying tissues.
Unless scar tissue is present, no need exists to remove any deeper tissues. Suture the skin with closely spaced sutures in a simple interrupted pattern using 4-0 or smaller suture material with swaged-on, cutting needles (Figure 4).



Upper eyelid entropion
Dogs with excessive facial skin folds, including the basset hound, bloodhound, Shar Pei and chow chow, may present with upper eyelid entropion. In these breeds, the upper eyelids “collapse” under the weight of the excess skin and, consequently, their eyelashes drop on to the cornea.
These patients are best treated surgically with the Stades procedure, named after the Dutch veterinary ophthalmologist who developed the technique. Unlike the modified Hotz-Celsus technique, here the first incision is made as close as possible to the eyelid margin, between the Meibomian gland openings and the upper lid eyelashes. The goal is to remove the eyelashes and their follicles, but avoid damaging the Meibomian glands.
The second incision will create a huge crescent of skin, sometimes 3cm to 4cm wide, which is removed. Rather than suturing the two incision lines to each other, the dorsal edge of the wound is sutured to the edge of the tarsal plate, approximately 4mm from the eyelid margin. This will leave an area of exposed subcutaneous tissue that will heal by second intention. The resulting scarring and contraction will result in additional eversion of the upper eyelid, and form a hair-free eyelid margin. More severe cases may be corrected by stellate rhytidectomy, modified brow suspension or other advanced procedures.
Lower medial entropion (brachycephalic ocular syndrome)
Many brachycephalic dog breeds suffer from an ocular brachycephalic ocular syndrome, which may include the following (Figure 5):
- Medial entropion of the lower eyelids. This causes kinking of the ventral nasolacrimal puncta and canaliculi, resulting in epiphora due to obstruction of the ventral tear drainage pathway. This may be further exacerbated by the ocular surface irritation caused by the medial entropion.
- The ocular surface may be further irritated by trichiasis of the medial caruncle, nasal folds and, most commonly, by breed-related lagophthalmos, macropalpebral fissure and shallow orbit, all leading to an exposed globe. These factors also predispose the dog to traumatic proptosis, discussed elsewhere in this article.
- These abnormalities contribute to pigmentary keratitis, which is further aggravated by tear film abnormalities seen in many of these breeds.
- Some clinicians may decide to remove the irritating nasal folds and/or correct the medial entropion. However, these may be only partial solutions that do not address the entire syndrome, which is best corrected by medial canthoplasty. The procedure includes:
- Cannulating the lacrimal punctas and cutting the canaliculi, thereby creating new punctas in the conjunctival lacrimal sac.
- Remove the medial caruncle and all of its hair follicles.
- Remove several millimetres (depending on the amount of lagophthalmos) of the upper and lower eyelid margins. Recreate the medial canthus with a figure-of-eight suture and two-layered closure. This will usually make nasal fold removal unnecessary, as they no longer come in contract with the ocular surface.
- Correct the medial entropion.
- Many dogs will require lifelong ciclosporin or tacrolimus treatment to address the tear film disorders and pigmentary keratitis.
Ectropion
Like entropion, ectropion (eversion of the eyelid) almost always affects only the lower eyelid. And, like entropion, it is most often conformational or breed-related ectropion, most frequently affecting breeds with loose facial skin, such as the spaniel, retriever, St Bernard and bloodhound.
Clinically significant ectropion is less common than entropion. In severe cases, the drooping lid exposes the ventral bulbar and lower lid palpebral conjunctiva, and impairs eyelid blinking, resulting in secondary lagophthalmos, keratitis or conjunctivitis.
Depending on the severity of the ectropion (Figures 6a and 6b), it can be resolved using one of the two following techniques.



Wedge resection (and repair of lid laceration)
The length of a normal eyelid is 33mm to 35mm. When mild ectropion is secondary to an elongated lower eyelid, you should shorten the lower eyelid by resecting a full-thickness wedge from the lateral end of the lower eyelid, restoring the eyelid to its normal length (Figure 5).
Next, a figure-of-eight suture should be used to achieve perfect alignment of the newly formed eyelid margin.
Finally, close the wound with a routine two-layer closure, making sure the sutures of the deeper layer are not full thickness, and do not irritate the globe.
The same suturing pattern (beginning with a figure-of-eight suture in the eyelid margin) should be used to correct traumatic lid laceration.
V-to-Y blepharoplasty
The V-to-Y (or Wharton-Jones) procedure is used for correcting moderate and severe, and cicatricial, cases of ectropion (Figures 6a and 6b).
Use a surgical marker to outline a triangle, its base parallel to the eyelid margin and its length extending along the everted part of the eyelid. Incise the skin along the two sides of the triangle, but not its base, forming a V-shaped flap of skin.
Dissect the underlying tissues, freeing this flap towards the eyelid margin, until the base of the triangle.
Next, begin suturing the incision at the triangle apex. Place simple interrupted sutures (4-0 or smaller silk or nylon) to appose the two sides of the triangle, forming a vertical suture line. This suturing pattern forces the base of the triangle and eyelid margin toward the globe.
The length of the vertical line is determined by the amount of eyelid margin elevation or inversion that is needed to correct the ectropion, adding another 2mm to 3mm to address wound contraction.
End the procedure by suturing the remaining arms of the two incisions to the free edges of the flap, forming a Y-shaped suture pattern.
Resectioning eyelid tumours
Full-thickness wedge resection is used to remove small eyelid tumours or (as aforementioned) to laterally shorten the eyelids in cases of mild ectropion.
When performing a wedge resection, the height of the triangle should be approximately twice its base. Make the skin incisions with a number 15 Bard-Parker scalpel while supporting the eyelid with a Jaeger eyelid plate (Figures 3a and 3b).
Cut the muscle, tarsal plate and conjunctiva with straight Mayo scissors, so that the tissue wedge is resected completely.
Appose the lid margin with a figure-of-eight suture and continue closure using the two-layered pattern.
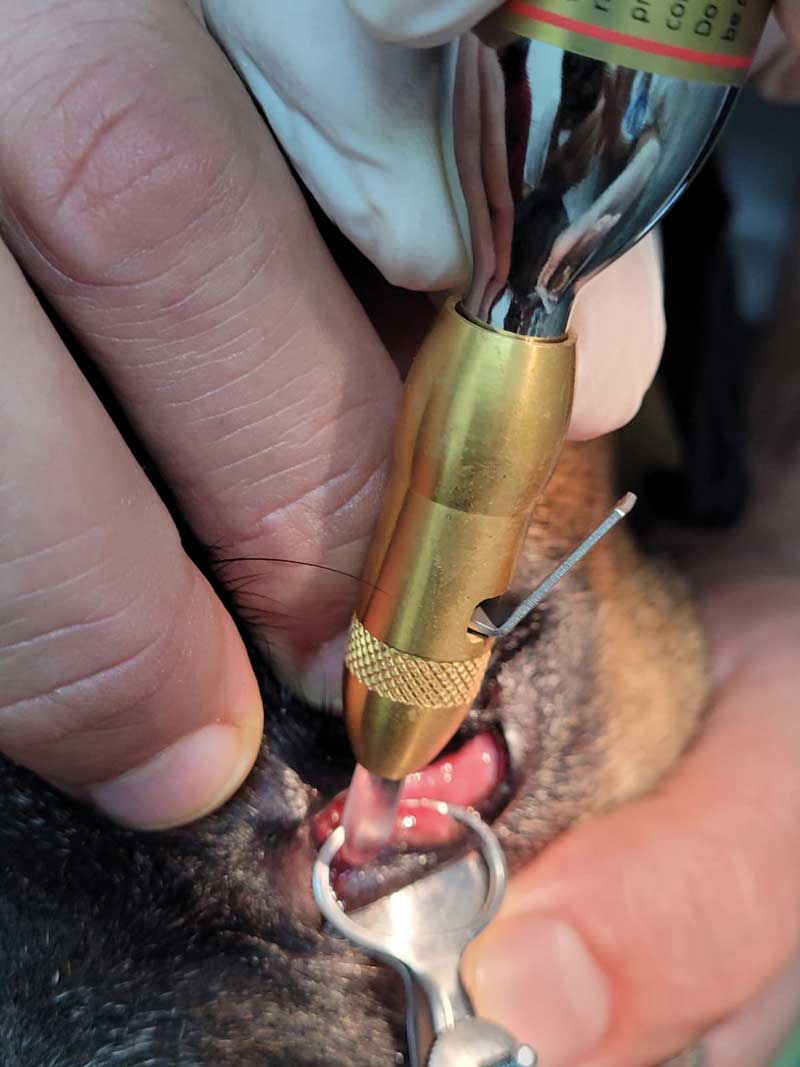
Alternatively, such small tumours may also be treated with cryotherapy (Figures 7a and 7b).
Tumours larger than 25% of the eyelid length in cats, and in mesaticephalic and dolichocephalic dogs, or more than 33% in brachycephalic dogs, should be removed using alternative surgical techniques such as H-plasty, house inverted triangle or other grafting techniques to reconstruct the eyelid (Figure 8). The reader is referred to surgery and ophthalmology textbooks for their detailed description.
- Use of some of the drugs in this article is under the veterinary medicine cascade.


Latest news
