12 Oct 2021
Cytology findings from a skin mass in a feline patient
Francesco Cian
Job Title
An 11-year-old female domestic shorthair cat presented for a long-standing 4cm solid interscapular mass, which had recently grown. The veterinarian performed a fine-needle aspirate (FNA) of the lesion and submitted the slides to an external laboratory for cytological examination.
The aspirate from the scapular mass showed a main population of mononuclear and slightly spindloid cells, either individual or arranged in small, poorly cohesive groups.
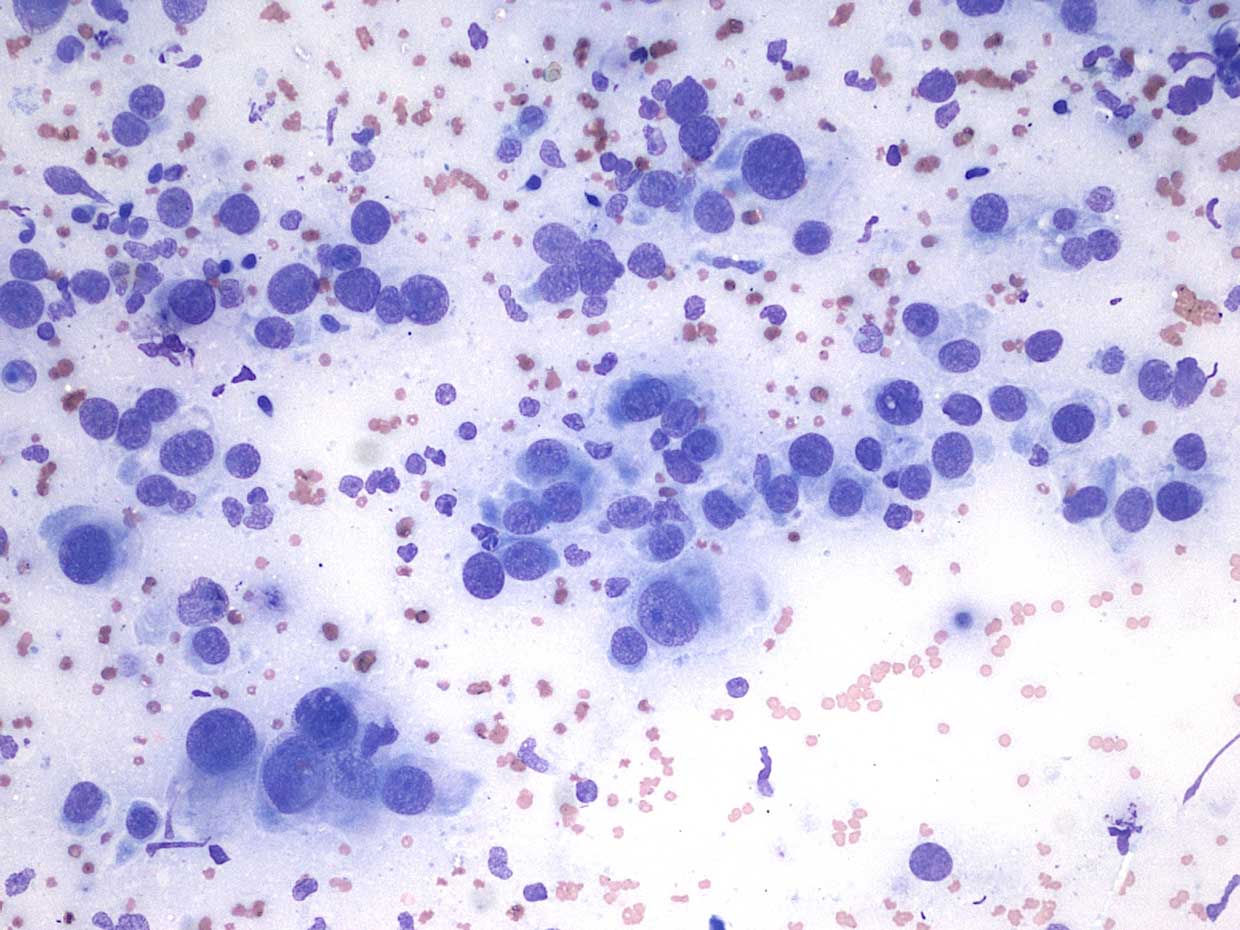
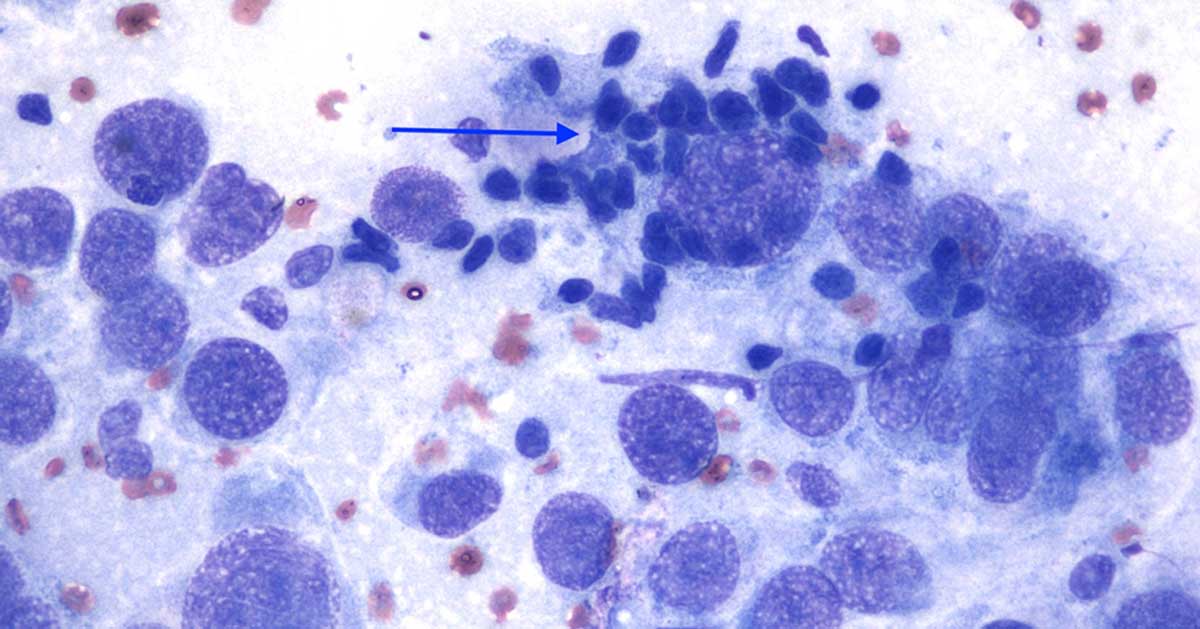
Cytoplasm is light blue (basophilic), with poorly defined and often slightly elongated borders. Nuclei are round to slightly oval and large in size, with granular chromatin and round nucleoli often visible. Anisocytosis (cell size variation) and anisokaryosis (nuclear size variation) are moderate to marked.
A few mitotic figures (not shown in these images) are present. Also, a few small lymphocytes (blue arrow) are present, and occasional segmented neutrophils, likely blood derived.
Diagnosis
The presence of a population of atypical spindleoid cells with features of atypia, together with the clinical history of a mass, were considered supportive of sarcoma.
In particular, the anatomic location of the mass (interscapular area) and the history of previous vaccination in the local area were highly suggestive of feline injection site sarcoma (FISS). Reactive fibroplasia was considered extremely unlikely.
Follow-up
After the diagnosis of sarcoma was reached, advanced imaging studies were performed, no metastases to regional lymph nodes or other organs were detected and the mass was widely excised accordingly. Histopathology confirmed the diagnosis of sarcoma, likely FISS.
Insight
FISS is a relatively uncommon malignant mesenchymal neoplasm that may occur in cats at sites of injections of different types of preparations (in particular, but not only adjuvated vaccines), microchip implants and non-absorbable suture material. It often presents as SC or IM, firm, often multilobulated and sometimes a fluid-filled mass of variable size. Based on a UK study (Dean et al, 2013), the incidence risk of FISS per year is low and was estimated to be 1/16,000 to 50,000 cats registered by UK practices.
These tumours are believed to arise from the neoplastic transformation of pluripotential mesenchymal cells present in the inflammatory and reparative processes following stimulus/damage. A genetic predisposition may also contribute to this.
FISS appears on cytology and histology with various lines of differentiation, from fibrosarcoma (the most common) to osteosarcoma, rhabdomyosarcoma or undifferentiated pleomorphic sarcoma. Features that are typical of FISS (but are not always present) include clusters of lymphocytes and plasma cells at the periphery of the tumour (as seen here), areas of necrosis and sometimes evidence of vaccine adjuvant within macrophages.
FISS behaves more aggressively than other sarcomas. It often has infiltrative growth with high recurrence rate. The rate of metastasis ranges from 10% to 28% and involves regional lymph nodes, lungs and other organs.
Pre-operative diagnostic imaging is crucial to identify potential metastatic disease and to establish the actual extension of the primary mass. Studies have shown that the actual size of tumours determined by CT could be twice that estimated at physical examination.
Treatment involves aggressive, radical excision and may be accompanied by preoperative or postoperative radiation therapy in selected cases. To facilitate wide amputation in the case of injection-site sarcoma, distal limb vaccine injection is currently recommended; more recently, ventral abdominal SC and tail injections have also been considered.
Take-home message
Diagnosis of sarcoma can be achieved on cytology, in particular in the presence of a main population of mesenchymal-looking cells with marked features of atypia and clinical evidence of a distinct mass.
Attention must be paid in the presence of concurrent inflammation or in the context of scar tissue/granulation tissue formation, since reactive fibroplasia may appear cytologically similar and reactive fibroblasts may display marked features of atypia, mimicking neoplastic cells. In those cases, histopathological examination is highly recommended.
The Vaccine-Associated Feline Sarcoma Task Force recommends that vets and owners monitor the vaccination site for swelling or lumps using the “3-2-1” rule.
Biopsy of any mass present is warranted if it (1) remains present three months after vaccination, (2) is larger than 2cm in diameter or (3) is increasing in size one month after vaccination. It is recommended to obtain an incisional biopsy on any masses meeting any of these criteria.
However, it is not uncommon among oncologists to start diagnostic work-up with a fine-needle aspirate, which in certain cases (as seen here), and together with the clinical picture, can provide a diagnosis of sarcoma, likely feline injecton site sarcoma, with a high degree of confidence.
References
- Dean RS, Pfeiffer DU and Adams VJ (2013), The incidence of feline injection site sarcomas in the United Kingdom, BMC Veterinary Research 22: 9-17.
- Hartmann K, Day MJ, Thiry E et al (2015). Feline injection-site sarcoma ABCD guidelines on prevention and management, Journal of Feline Medicine and Surgery 17(7): 606-613.
- Roccabianca P, Schulman FY, Avallone G et al (2020). Surgical Pathology of Tumours of Domestic Animals: Tumours of Soft Tissue (Volume 3): 108-112.
- Stone AS, Brummet GO, Carozza EM et al (2020). 2020 AAHA/AAFP Feline Vaccination Guidelines, Journal of Feline Medicine and Surgery 22(9): 813-830.