6 Mar 2023
Resolution of an unusual oesophageal foreign body
Greg Steele MA, VetMB, MRCVS and Peter Chalkley BVSc, MRCVS share a unique case that highlights the need for adaptability in practice

Figure 1. Initial lateral survey radiograph of thorax and abdomen, showing multiple radio-opaque foreign bodies.
A Jack Russell terrier was presented to a first opinion practice with a history of chewing a skirt, and investigations revealed an oesophageal foreign body. This was found to be the slider of a zipper from the skirt, into which the walls of the oesophagus had become doubly embedded.
Referral was offered, but declined, so the veterinary team used initiative and a “thinking outside the box” approach to solve the unique problem and deliver a good outcome. The investigations, approach to the problem and follow-up are described in detail.
This is presented as an interesting case, but also a good example of what can be achieved with the diverse skill set of the modern veterinary team.
Background
This report describes a highly unusual and unexpected situation in which a zipper mechanism had zipped into the walls of the oesophagus and formed a very challenging oesophageal foreign body. Through unusual methods, a successful outcome was achieved.
The authors are presenting this case as a good example of the diverse transferable skillset of the modern veterinary team, and an example of using initiative in a novel circumstance to achieve goals. This also emphasises the importance of pragmatically doing one’s best where the gold standard is not available.
Investigation and treatment
The Jack Russell terrier presented to the practice for consultation with an 18-hour history of violent retching and vomiting. The dog was a neutered male, aged eight years and five months old, with no other significant health problems other than occasional mild colitis (transient fresh blood in faeces), which responded to symptomatic treatment.
The dog had a history of slug pellet (organophosphate) ingestion as a puppy, which was treated with supportive hospitalisation and the dog made a full recovery. It was fully vaccinated.
The dog had eaten normally the night before, and on the morning of the consultation, but regurgitated/vomited immediately afterwards on both occasions. The owners reported choking and retching associated with this, but the dog was bright and alert throughout. No cough or sneeze were present. The dog was a known scavenger and the owners had found a chewed skirt that morning, with the zip damaged.
On presentation, the dog was bright, alert and responsive – and extremely excitable. Mucus membranes were pink and moist, with a normal capillary refill time of less than two seconds. On thoracic auscultation, the heart and lungs were within normal limits, with a heart rate of 148 and largely panting respiration. The throat was evidently sore on palpation and a throat-clearing noise could be elicited. The abdomen was non-painful and unremarkable on palpation, and the dog was normothermic.
Based on the history, a strong suspicion existed of a foreign body being the origin of the clinical signs. Other differentials included soft tissue trauma in the throat, gastroenteritis and pancreatitis. A decision was made with the owners to sedate the dog to examine the throat and perform a radiographic investigation. Blood samples were not taken in the first instance as pancreatitis and gastroenteritis were deemed to be less likely differentials. The previous history of colitis was not relevant at this stage.
An IV line was placed and the dog was sedated intravenously with medetomidine (20µg/kg) and buprenorphine (0.02mg/kg). On visual inspection, the throat and epiglottis were normal. Right lateral and dorsoventral thoracic and abdominal radiographs were then taken. A composition image is displayed (Figure 1).
The imaging identified oesophageal (dorsal and caudal to the heart base), gastric and intestinal foreign bodies, likely of metallic origin. The intestinal bodies were decided to be of lesser importance based on their further extent of passage. The clinical signs were most likely explained by the oesophageal and gastric foreign bodies. The owner was updated, and permission was given for general anaesthesia and endoscopy.
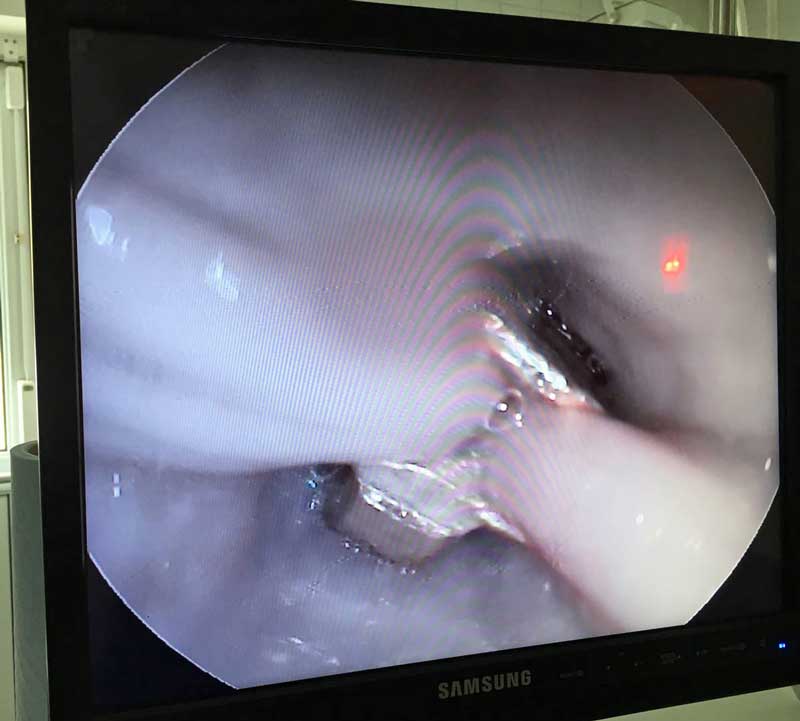
The dog was induced with propofol (1mg/kg) intravenously and an endotracheal tube was placed. It was maintained routinely with isoflurane and endoscopy was performed. The foreign body in the oesophagus was identified as the zipper slider itself, from a zip on the skirt (Figure 2). The slider had efficiently captured the walls of the oesophagus in its structure on both sides, just as it is designed to function during closure of a garment. This, unfortunately, had very firmly wedged the zipper in the oesophageal mucosa, and no movement could be achieved with the endoscope or associated tools. The mucosa did not appear to be heavily damaged, but inflammation was present where it was captured by the sides of the zipper.
The level of interaction between zip slider and oesophagus was likely achieved by oesophageal motility and peristalsis, and indeed, two short parallel lines of inflammation were visible just cranial to the zip slider, where it had likely started its journey.
At this stage, the owners were updated and, based on the risks associated with oesophageal trauma and potential rupture, were offered referral to a local specialist centre that had already offered advice over the telephone. Oesophageal damage and its sequelae were both discussed at length with the owners. Referral was declined based on financial constraints, and the dog was uninsured.
On further discussion, the owners requested that continued removal of the zipper be attempted despite the high risks associated, on the basis that should rupture occur or should removal be impossible, the dog be euthanised while still under general anaesthesia. Socially and ethically, this was a difficult decision, but the alternative of euthanasia was extreme, and the dog’s welfare was believed to be safeguarded by general anaesthesia throughout. The team and the owners agreed that it was worth the risk to attempt to save the dog’s life.
An effective review of all common methods for oesophageal foreign body removal, including all those discussed below, is provided by White1. Options were considered, and it was decided to try moving the zipper down the oesophagus towards the stomach, where it could be retrieved by gastrotomy. Further attempts with the endoscope and its basket were unsuccessful: trying to retrieve it orally was hindered by difficulty gripping the zipper and by the shape of the design, which seemed to oppose any further movement in that direction.
The mucosa could not be easily extricated from within the zipper structure. The use of a Foley catheter passed beyond the object has been described, but was not considered in this case based on the lack of any movement orally and the inevitable loss of good visualisation during traction.
Eventually, the zipper did start to move down the oesophagus with a combination of large diameter tube and the endoscope. The endoscope was placed inside an equine stomach tube and the zipper visualised, and then the rim of the stomach tube was used to slowly edge the zipper down the oesophagus and away from the mucosa. A much larger diameter small animal endotracheal tube also provided a good alternative due to the tapered shape of the end.
A combination of pushing and rolling the tube allowed the authors to edge the zipper away from the mucosa and down towards the stomach. This took some time, but eventually it was judged to be close enough to the stomach. The oesophagus was reassessed at each stage, and no major rupture or damage to the mucosa was noted.
Some inflammation and bleeding was observed in the mucosa, but nothing that seemed more than superficial. Based on this assessment, post-endoscopy radiographs to assess the mediastinum were not performed, but would be indicated if evidence existed of greater damage to the oesophagus. Again, the owners were updated, and permission was given for gastrotomy.
A routine celiotomy was performed. The stomach was visualised, stay sutures were placed and laparotomy swabs packed around it. A large incision was made along the greater curvature. A ceramic foreign body was initially retrieved from the body of the stomach (Figure 3).

The stomach itself appeared healthy. Digital exploration of the oesophagus allowed the detection and retrieval of the zipper, which detached from the oesophageal mucosa without too much difficulty. The stomach was closed routinely. The rest of the abdomen was inspected and appeared normal. The remaining foreign bodies were found in the colon and deemed not worthy of retrieval at that stage. The abdomen was flushed and closed routinely.
Perioperatively, the dog was given IV fluid therapy (Hartmann’s solution), methadone (0.3mg/kg), paracetamol (10mg/kg), amoxicillin (8.75mg/kg), metronidazole (IV solution 10mg/kg), omeprazole (IV solution 1mg/kg) and ranitidine (IV solution 2mg/kg), and these were continued postoperatively.
Dual first-line antibiotic therapy with gastroprotectants were chosen based on the gastrotomy and damage to the oesophagus. Sucralfate is indicated in these cases1, but was unavailable. Hospitalisation and intensive monitoring were continued overnight and into the next day. No complications occurred with recovery other than hypothermia, which resolved with use of a warm air blanket.
Blood samples were taken perioperatively and postoperatively to monitor biochemistry (including lactate and electrolytes, especially), but these displayed no major abnormalities.
Follow-up
The dog was hospitalised for a further 24 hours before seeming comfortable, bright and alert, and starting to show interest in food. At this point, it went home, continuing with oral medications of co-amoxiclav (12.5mg/kg twice daily), metronidazole (10mg/kg twice daily), omeprazole (1mg/kg twice daily), ranitidine (tablets 2mg/kg three times daily), paracetamol (10mg/kg three times daily) and tramadol (capsules 2mg/kg three times daily).
At first review two days post-discharge, the dog was eating small amounts with difficulty when hand-fed and drinking well. No vomiting was reported and medications were being given well. The surgical incision was healing well with no concerns. Vital parameters were within normal limits.
At seven days post-discharge, the dog was much improved, bright and alert, and passing normal faeces. Vital parameters were normal and the abdomen was comfortable. Healing was proceeding well. Eating was still with signs of discomfort and not to a normal level, but improving daily.
By this follow-up, the dog was eating without overt encouragement.
An unexpected visit was made 10 days post-discharge where he had passed some fresh blood in normal faeces. The clinical examination was normal and the dog was otherwise well. The anal glands were both very full of normal contents and easily emptied. This was deemed to be a flare-up of the dog’s previous colitis condition, related to the stressful circumstances in the past 10 days and not likely to be of relevance to the foreign body management. No additional treatment was given and the blood resolved quickly.
By 14 days post-discharge, the dog was assessed to be more or less normal and eating well. Eating was slower than normal, but enthusiastic and daily intake was back to a full amount. All oral medications were finished off by this postoperative check. The surgical incision had healed completely with no concerns. The dog was signed off and invited to return to normal, including a gradual return to exercise. Routine follow-up was also scheduled to monitor for stricture formation.
Retrospective research has indicated a long-term rate of up to 25% of oesophageal foreign bodies leading to strictures, but have suggested a full recovery in 72% of dogs2,3. Strictures are suggested clinically by the regurgitation of any food not mashed beforehand2. The owners were requested to be vigilant with any potential foreign bodies in the future.
Discussion
The authors could find no published reports of a similar foreign body in the literature, but oesophageal foreign bodies in dogs and cats are common emergencies presented to first opinion practitioners. Only one related example was found from human medicine, which involved a similar foreign body in the trachea of a young boy4.
- Always be ready for the unprecedented in first opinion practice.
- Where the gold standard option is not available, don’t be afraid to proceed pragmatically, using your initiative and transferable skills.
- The veterinary team is extremely skilled in making the best of a situation and thinking outside the box under time pressure – have faith in that and it will often reward you.
- Communication is essential. Good dialogue between the team and the owners in this case was vital to relay facts, plans and potential hazards at every stage.
- Research suggests that cases of oesophageal foreign body have at least a 70% chance of a positive outcome where appropriately managed.
One veterinary case that was endoscopically removed was described by The University of Edinburgh as a case study5. This case study succinctly summarises a similar approach to removal as employed here, but with successful oral retrieval rather than gastrotomy.
A retrospective study of 44 dogs presented to University College Dublin has also provided good data on factors affecting success in retrieval and long-term outcomes2. This paper is used for reference previously in the text.
Fittingly, middle-aged terriers were over-represented in this study and the authors’ report lends further evidence to this data. The authors of that study noted a tendency for terriers to have foreign bodies caudal to the heart base (as in our study), which may be breed‑associated and be based on oesophageal motility.
Concerns could be raised ethically over the decision-making in this case based on financial decisions. Unfortunately, this is the reality of private veterinary practice. The team involved in this study felt that euthanasia on financial grounds was difficult to accept in this case, and because the animal was maintained on pain relief and general anaesthesia, animal welfare was not thought to be threatened at any stage. The risk of attempting more aggressive removal of the foreign body was worthwhile to avoid euthanasia, but euthanasia was kept as a last resort to avoid suffering and distress.
This decision was reached with the agreement of the owners and the practice team, and in the end, the outcome was the best one that could have been hoped for.
At a time when the role and value of general practice is a big talking point for the profession, the authors hope cases like this demonstrate the skills and adaptability that first opinion practice can still offer.
Use of some of the drugs mentioned in this article is under the veterinary medicine cascade.