9 May
The power of cytology: regional lymphadenomegaly in a dog
Francesco Cian
Job Title
An eight-year-old female Labrador retriever was presented to the veterinarian for rapid onset unilateral facial swelling. The dog had a history of a small (1cm × 1cm) cutaneous lesion on the lip present for the past six months.
As part of the initial diagnostic workup, the veterinarian performed a fine needle aspirate of the lip lesion, which was supportive of mast cell tumour (MCT), ultrasound of the facial swelling and aspirate of the enlarged left submandibular lymph node.
Pictured are images of a left submandibular lymph node in an adult dog, fine needle aspirate (Wright-Giemsa, 20× to 100×).
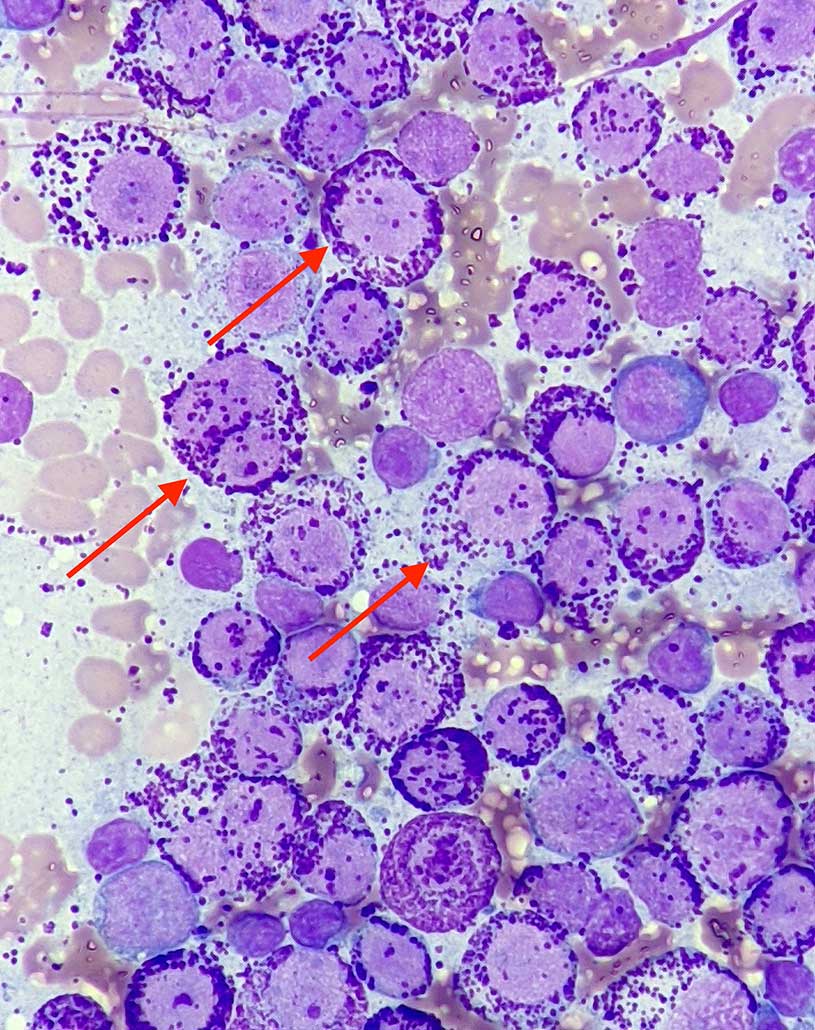
The lymph node aspirate was highly cellular and well preserved. The background appeared clear with red blood cells and some free purple granules. A main population of mast cells was observed (red arrows), characterised by numerous purple/magenta granules, often filling the cytoplasm and partially obscuring nuclei.
Those, when visible, were round, paracentrally located, large in size, with granular chromatin and round nucleoli sometimes visible. Anisocytosis (cell size variation) and anisokaryosis (nucleus size variation) were moderate, and rare binucleated cells were observed.
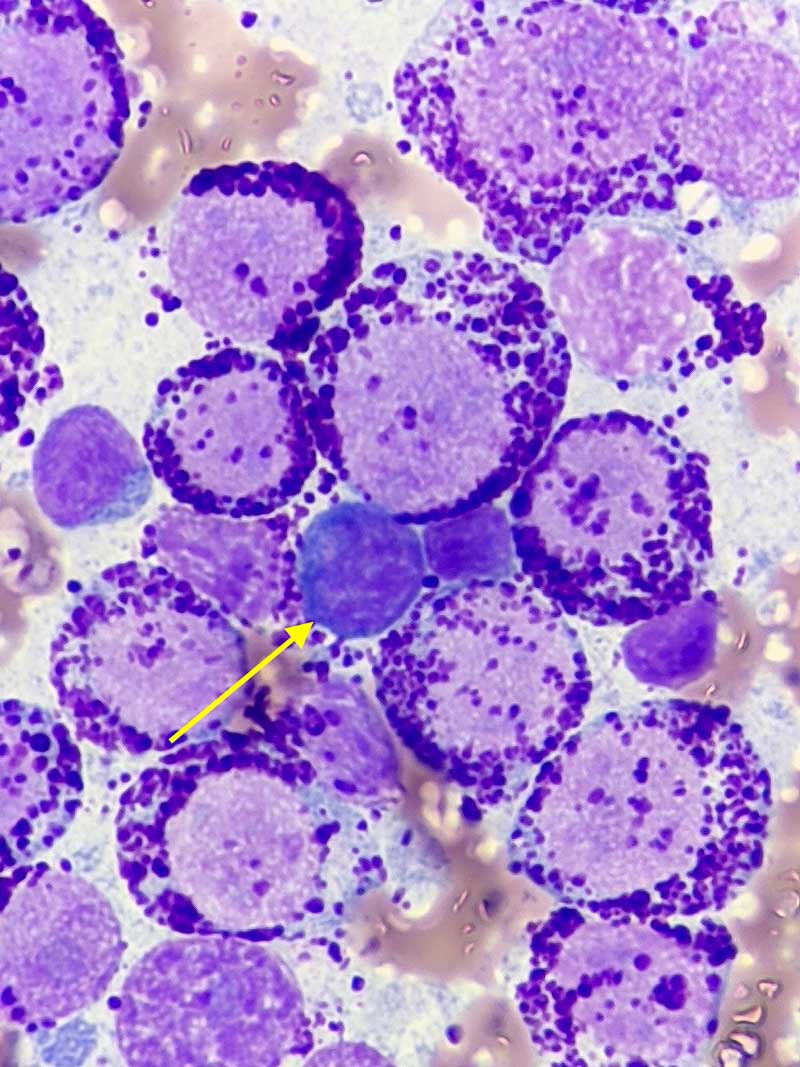
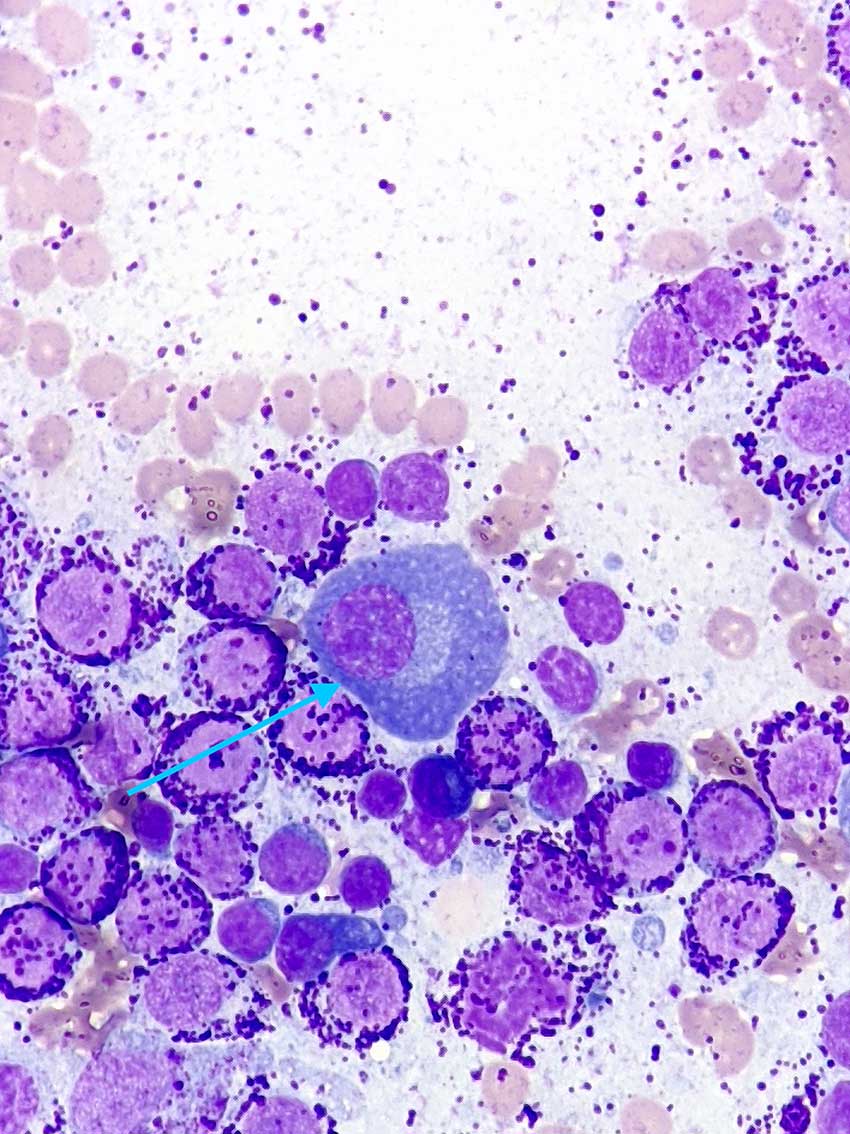
Few lymphoid cells (yellow arrow) and plasma cells (light blue arrow) were also noted, suggesting some degree of concurrent reactive lymphoid hyperplasia.
Diagnosis
A diagnosis of metastatic MCT was made.
Follow-up
Full clinical staging revealed involvement of both submandibular and prescapular lymph nodes, but not metastatic disease at the level of internal organs, bone marrow/peripheral blood.
Given that it was not possible to perform surgical excision due to the extension of the tumour, the dog started treatment with prednisone and vinblastine. He also received radiotherapy to the muzzle and neck (primary and drained lymph nodes) over four consecutive weeks.
A partial (almost complete) remission was obtained and maintained for four months. The protocol was then switched to oral lomustine as recurrence of the metastatic disease became apparent. The dog died from sudden onset of respiratory distress 6 months after starting specific treatment and 12 months after the appearance of the lip lesion.
Insight
MCT is a very common neoplasm of dogs, accounting for 16% to 21% of skin neoplasms. It is mainly cutaneous; however, SC and visceral forms have also been described.
It is often solitary, although a significant proportion of dogs present with multiple tumours. It has been reported in dogs of any age and sex, with older subjects being more often affected. Selected breeds (for example, boxers, retrievers, pugs, Boston terriers and pit bull terriers) are at a higher risk.
Canine cutaneous MCTs have highly variable clinical behaviour, and histologic grading is considered the best method to predict biological behaviour. This includes a three-tier grading system by Patnaik et al that divides MCTs into well-differentiated, intermediately differentiated and poorly differentiated forms.
Although this grading system has been referenced widely by pathologists when providing a histologic grade, over the years a high degree of inconsistency has occurred in accurately applying the criteria of this grading system, and the reproducibility of assigned grades has been poor among pathologists.
Moreover, cases assigned as intermediately differentiated have showed very variable and unpredictable clinical behaviour. A two-tier histologic grading system by Kiupel et al was then established to increase interobserver consistency and also to identify more accurately those MCTs that have a high risk of aggressive biological behaviour. Both systems are used by veterinary anatomic pathologists to grade canine cutaneous MCTs.
Evaluation of metastatic disease in lymph nodes is more challenging on both cytological and histological point of views since universally accepted criteria have not been established.
A study by Krick et al provided cytological criteria to evaluate metastatic disease in lymph nodes.
This is based on the subjective number of mast cells in the sample, their degree of atypia and granulation, and their tendency to form cell aggregates.
Metastatic disease can be present even in the absence of lymphadenomegaly, underlying how lymph node palpation alone is a poor predictor of metastasis and how microscopic evaluation of the lymph node is of paramount importance.
Take-home messages
Grading canine cutaneous MCTs can be attempted by cytology; however, histopathological examination after mass removal is always recommended to confirm these findings.
Cytology of regional lymph nodes should always be performed as part of clinical staging for MCTs, regardless of their size, as metastatic disease is often, but not always associated with lymphadenomegaly.
- Drugs mentioned in this article are used under the cascade.